To arrange a free 30-min consultation, please email
enquiries@traumaform.hush.com
PTSD & Complex Trauma
“Traumatized people become “stuck” in the horror they endured. Traumatic memories dominate the life of many survivors, who continue to live in fear and feel tormented, even when the threat is long gone. Their body and mind feel and act as if an ongoing threat endangers their survival. At the core of psychological trauma is the confusion of past and present.”
Schauer, Neuner & Elbert, 2005
Types of Trauma Symptoms
Generally practitioners may distinguish between Simple and Complex Trauma, or PTSD I and PTSD II.
PTSD I may develop after a single incident or multiple single incidents such as a Road Traffic Accident (also known as a “large T”), and is largely fear-based.
Complex Trauma can develop as a result of prolonged and repeated incidents where an individual knew these would re-occur, but was helpless and horrified and unable to stop it from happening. Examples of this are witnessing or being the victim of domestic violence or emotional, physical or sexual abuse, or neglect, during childhood (also known as “little T’s), with the emotions typically occurring being anger, shame, grief, guilt and disgust.
There are numerous symptoms commonly associated with these, some of which may occur soon after the trauma and some develop over time.
The DSM (Diagnostic and Statistical Manual of Mental Disorders) is the reference manual that is used by psychiatrists and other health professionals to diagnose mental disorders and was created by the American Psychiatric Association.
It was first published in 1952 and not until 1980 was PTSD (Post-traumatic Stress Disorder) added.
Since then there have been various changes over the years.
The DSM 5 does not distinguish between PTSD and Complex Trauma.
The major 4 categories include:
Re-experiencing the event
— this can be in the form of spontaneous memories of the traumatic event, reliving the event as if it were happening now, recurrent dreams or nightmares related to it, flashbacks or other intense or prolonged psychological distress.
Hyper-arousal
— sometimes reckless or self-destructive behaviour, aggression, sleep disturbances, hyper-vigilance, shallow breathing or racing heart or related problems.
Avoidance
—trying to push away or avoid any distressing memories, thoughts, feelings or external reminders of the event.
Negative thoughts and mood or feelings
— this could be feeling numb, blaming oneself or others, feeling distant and cut off from others, loss of interest in previously enjoyable experiences, and inability to remember aspects of an event.
The DSM 5 also added a new category known as PTSD Dissociative Subtype - Symptoms of Dissociation include feeling that the world around is not real or seems distorted, detachment from one’s own body, dreamlike states and de-personalisation.
Dissociation is common in survivors of Type II trauma as it serves as a coping mechanism when a person is unable to fight or flight.
Symptoms of PTSD
Symptoms of Complex PTSD
- Chronic difficulties in emotion regulation and compulsions, anger and rage, self harm and suicidality, impulsive behaviour and risk taking;
- Alteration in attention or consciousness as in amnesia, dissociation and/or depersonalisation, including Dissociative Identity Disorder
- Somatisation can include chronic pain, problems with the digestive system, fatigue, cardiopulmonary symptoms, headaches, nausea
- Alteration of self-perception – a sense of self characterised as feeling defective, like a failure, chronic shame and guilt, self blame, feeling alone and misunderstood
- Alterations in perception of the perpetrator – a distorted view of the perpetrator, such as idealisation, distorted beliefs or obsession with causing perpetrator harm
- Difficulty with interpersonal relationships – lack of trust, vulnerability, withdrawal, revictimisation or victimising others
- Alteration in systems of meaning such as faith, a sense of hopelessness and despair.
Dissociation
- Amnesia: Can’t remember incidents or experiences that happened at a particular time, or can’t remember important personal information.
- Depersonalisation: A feeling that your body is unreal, changing or dissolving. Out of body experiences such as seeing yourself watching a replay.
- Derealisation: World seems unreal. May see objects changing in shape, size or colour.
- Identity Confusion: Uncertain about who you are or struggling to define self.
- Constriction: Our awareness of events is blunted, as well as our emotions. A person will have a hard time focussing or concentrating, will see and hear less clearly, and be easily distracted.
- Withdrawal and Avoidance: A person will withdraw more, perhaps becoming socially isolated, and put a lot of energy into avoiding reminders of the trauma.
- Detachment: Time seems distorted and people are not aware of their boundaries so they can be clumsier and be injured easily.
- Rigidity: Sometimes in order to cope, people will gravitate to the other extreme of being super-organised and seem over-controlling of oneself and/or others.
Traumatic experiences shake the foundations of our beliefs about safety, and shatter our assumptions of trust
In order for the experience of an event to be traumatic it does not have to directly affect a person - witnessing or even hearing about an event can be considered to be exposure to a traumatic event. It is often the meaning or perception of the event that is more significant than the actual severity of incident.
Often people cope in very different ways, some coping strategies or coping behaviours may be more effective than others…. In other words, trauma is defined by the experience of the survivor.
Two people could undergo the same noxious event and one person might be traumatised while the other person remained relatively unscathed.
Some people can be high achievers and high functioning yet suffer the effects of Complex Trauma throughout their life, and might not even be aware of this. Others have more developed symptoms of PTSD and may have other co-occurring disorders such as self-harm or addictive behaviours in order to help them cope.
Some people may have no family or support system and may be homeless. Most people experience a sense of isolation and aloneness.
Most people who are exposed to trauma will experience a stress reaction – this is entirely normal as our bodies through years of evolution developed the fight-flight or freeze response.
Does Everyone Develop PTSD?
It is estimated that roughly between 10 and 20% of people exposed to a traumatic event will subsequently develop PTSD. Researchers are busy trying to elicit what pre-disposing factors may influence its development.
Some things that increase the likelihood of developing PTSD are:
- Freezing in response to trauma – those who become immobile in the face of severe threat as an instinctive survival technique
- Previous history of trauma
- Greater distress at the time of trauma and immediately thereafter
- Dysfunctional family
- Pre-existing psychological disorder
- Poor coping skills
- Age – younger or older people are at greater risk
Whereas most people recover from trauma after a period of time, a small minority go on to develop symptoms of PTSD, which can be of varying intensity, some may lead to minor difficulties whereas severe symptoms can be severely debilitating in every area of life.
PTSD is treatable. There are a number of interventions available that have been shown to markedly reduce or even eliminate the symptoms of PTSD.
This is not a condition you need to live with forever.
Although we cannot change history, we can change the way your history affects your life now. You can recover from your traumatic experience(s).
Trauma symptoms are probably adaptive, and originally evolved to help us recognise and avoid dangerous situations
Complex PTSD and Attachment
Later Symptoms
Co-occurring disorders
Anxiety
Anger
Guilt and Shame
Depression and Low Mood
Addiction and Substance Use
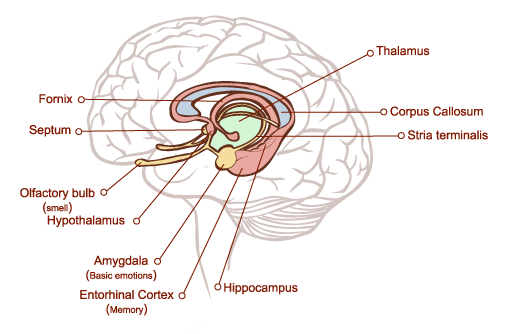
A bit about the brain
The Brain Stem
The brain stem (also referred to as the reptilian brain) sits at the base of the brain and regulates such functions as reflexes, sleeping, our temperature and breathing. In evolutionary terms it is the oldest part of the brain. Lizards and other reptiles have a brain stem which regulates these activities but their brains did not develop much further than that.
The Neo Cortex
The Limbic System
Fight, Flight, or Freeze
Fees
Fees can be discussed in the initial informal chat.
Please don't be afraid to ask about concessions at any point during therapy as situations may change.
Copyright attributions: Sisters with Kite by senivpetro on Freepik; Fees Image: Close-Up Almond Blossom by Freepik
Contact Details
enquiries@traumaform.hush.co.uk
Trauma Therapy
Aberystwyth, Carmarthen, Lampeter, Swansea, Daytime, Evenings and Weekends